THE MAUREEN DESMOND FOUNDATION

Over the years, The Mater Hospital provided incomplete records to The Dublin City Coroner, incomplete records to The Medical Council, failed to provide complete records in requests for voluntary discovery of records, failed to provide complete records in response to an order for full-discovery of records made by The High Court, and failed to meet its promises made in relation to a motion for further & better discovery of records filed in The High Court, failed to respond to multiple Freedom of Information requests seeking records, documents & information including requests for further details of why the amount of recorded complaints against the gynaecology area at The Mater Hospital spiked significantly in 2010 and 2011 at the same time as Maureen's late-diagnosis & death. The hospital has not responded to requests to clarify if any of these recorded complaints relate to the late-diagnosis of gynaecological cancers.
In the long-running aftermath of the inquest which saw the Dublin City Coroner issue a verdict of medical misadventure in the death of Maureen Desmond (click here for Death Certificate: CERTIFICATE), her family returned to The High Court on February 17th 2020, for a third time, to try to get The Mater Hospital to release all of Maureen Desmond's remaining medical records and related files & documents. The Mater failed to release a complete set of files and documents after the High Court ordered a full release in 2018.
Click here for a list: MISSING RECORDS, FILES AND DOCUMENTS.
_______________________________________________________
A full independent medical report into the gynaecology care Maureen received at The Mater Hospital is available below--please scroll down. The report written by world-leading gynaecologist Dr. John Monaghan cites negligence and failure in duty of care. The report was submitted to the inquest into Maureen's death by her son Stephen, and as such forms part of the public record of the inquest. The report concludes: "In my view there was clear evidence of a breach of duty of care in this case. In causation terms, if Mrs Desmond had had a diagnosis of her uterine cancer made some one year and eight months prior to its eventual diagnosis she would have had a simple procedure such as a total hysterectomy with removal of ovaries and on the balance of probabilities would have been cured of her cancer. Uterine cancer has a very high cure rate when the cancer is diagnosed within the confines of the uterus but the cure rates drop rapidly when spread has occurred outside the uterus. It is a pity that the opportunity to diagnose this cancer at an eminently curable phase was lost due to the failings of the Mater Hospital and its staff ."
Please scroll down for the full report...or click on this link: MEDICAL REPORTS
After an extensive investigation The Dublin City Coroner Dr. Brian Farrell issued a verdict on the 26th September 2014 of Medical Misadventure in Maureen's death. Maureen Desmond's family are now waiting on a full apology from The Mater and the HSE.
In summary below, please see a list of medical incidents which were reported by the author of this site at the inquest into the death of Maureen Desmond, together with a description of relevant events and outcomes at the inquest. The medical incidents included below are reproduced here from the transcript of testimony & evidence given at the inquest. The transcript is a public document and available at The Coroner's Office. The author of this website also retains the audio recordings of the inquest created by The Coroner's Office, which are also a matter of public record. We have chosen not to name any of the treating-doctors in our writing and original paragraphs on this website, even though we are perfectly entitled to do so in the context of providing a report in relation to an inquest.
Maureen was late diagnosed with uterine cancer by 2 years. She had been discharged from the gynaecology clinic at The Mater Hospital by a junior doctor without completing a scheduled biopsy and without follow-up on her symptoms. The coroner ruled that this incident at The Mater was a "missed opportunity" to diagnose Maureen with cancer, and that this treatment-episode constituted a "risk factor" for patient safety. Maureen subsequently attended 28 outpatient appointments in other clinics at The Mater in an effort to establish the nature of her illness. She was diagnosed with irritable bowel syndrome but was found shortly after that to have late stage uterine cancer. At the inquest, it came to light that a CT colonogram which Maureen had at the Mater was read as 'normal' by some of the the Mater radiologists. Experts for the coroner found cancer on the same scans in question. The coroner ruled that this incident at The Mater was a second "missed opportunity" to diagnose Maureen with cancer, and that this treatment-episode constituted a second "risk factor" for patient safety. While on chemotherapy, Maureen was administered a double dose of Carboplatin at the same time as she was administered a maximum dose of Taxol. She experienced anaphylactic shock. Maureen was also found to have a life-threatening 'central line infection' in a port that was fitted to administer chemotherapy. Central line infections are usually considered preventable with proper aseptic installation techniques at the hospital.
Maureen spent her final week in the Mater with an undiagnosed pulmonary embolism (a clot). During this stay in hospital Maureen was administered fluids under the skin on her stomach (lower abdomen) because a doctor had failed to insert a cannula into her vein. As a result, Maureen's abdomen filled with water and became massively distended. The fluid was drained through a surgical procedure. In the the last 24 hours of her life, when the hospital finally diagnosed her as having an embolism, Maureen, who was entirely coherent, made it clear directly to medical staff that she wanted every possible intervention to save her life. At the inquest her palliative care consultant doctor, from St Francis' Palliative Care, who had seen Maureen at home shortly before her final admission to the Mater, indicated that Maureen's death was not in any way imminent from her cancer, that she was not experiencing any pain or taking any significant pain medication at home, and was mentally alert and in good spirits. The night she died Maureen had been waiting 24 hours for transfer from the open wards at The Mater into the Special Care Unit (which is a kind of ICU at the Mater), for treatment of her pulmonary embolism. Beds had been unavailable that night in the Special Care Unit. During this waiting-time Maureen was administered--without her knowledge, wishes or consent--lethal levels of morphine. This was evidenced in the autopsy-toxicology results presented at the inquest. The coroner's histopathologist at the inquest offered to officially record and list 'morphine-toxicity' as a secondary cause of death on Maureen's autopsy report--(a point documented in the official minutes of the inquest and by the journalist from Village Magazine who followed the proceedings. Click for article-see second last paragraph.) Maureen died just as a bed finally became available for her in the Special Care Unit after a 24 hour delay, i.e. while the doctor was preparing her for transfer to the SCU, Maureen experienced respiratory & cardiac arrest. A full attempt was made by the medical staff to resuscitate Maureen which ultimately failed.The coroner ruled that there were two distinct opportunities to diagnose Maureen with cancer which were missed by the hospital. The coroner pointed out that it was not his statutory remit to establish clinical negligence, or individual wrongdoing, but it was his statutory remit to highlight risk factors to patients' lives which could have been avoided. His position is detailed very clearly in this article in Village Magazine by a journalist who followed the inquest very closely: Click for article. The Coroner's ruling indicated that when the Gynaecology Registrar at The Mater discharged Maureen outright from the gynaecology clinic even though the findings of his hysteroscopy were fully at odds with the findings of the scans, without obtaining a biopsy, without any further investigation or follow-up, this in fact constituted a clear missed opportunity to diagnose Maureen and potentially save her life. The Coroner's ruling also indicated that a subsequent CT colonogram which showed cancer and was read at The Mater as 'normal' also constituted a clear missed opportunity to diagnose Maureen and potentially save her life. The coroner noted that Maureen was 'still operable' at the time the CT Colonogram was taken. For the coroner, these medical practices represented "risk factors" for patient safety. Since the inquest, The Mater Hospital and the HSE have not apologised to the family of Maureen Desmond, in spite of repeated requests to do so, nor have they come forward with or published any remedies they have instituted to the risk factors to patient safety identified by the Dublin City Coroner in this case.
Please note: that in the description above we do not identify, nor seek to identify any specific doctor since it is not our goal or intention to do so in any of the original statements and writings of Stephen Desmond & The Centre for Conflict Resolution Journalism, included on this website.
(See transcript of inquest for documentation of all the points made above-The full transcript of the inquest will soon to be available online on this website). Statements made by the author of this site in the above paragraph and elsewhere, should be understood as a "statement in report of the inquest or trial", and / or "an accurate report and statement-summary of a statement made during and/or connected with proceedings before a coroner, or judge."
INDEPENDENT MEDICAL REPORT BY WORLD-LEADING GYNAECOLOGIST INTO THE CARE PROVIDED TO MAUREEN DESMOND AT THE MATER HOSPITAL CITES NEGLIGENCE AND FAILURES IN DUTY OF CARE
Please note that this medical report was submitted by Stephen Desmond to the Inquest into Maureen Desmond's death conducted by The Dublin City Coroner, and as such is part of the public record of this inquest--and it is provided here as part of that public inquest record, and the accurate reporting of an inquest. See full disclaimer at the bottom of this page.
MEDICAL REPORT
Prepared by
Mr J M Monaghan, M.B, FRCS(Ed)., FRCOG
Consultant Gynaecological Surgeon
in the matter
of
Mrs Maureen Desmond
Date of Birth: 26.06.1937
Date of Death: 04.09.2011
Requested by
David Harris, Solicitor.
Ivor Fitzpatrick & Company,
44-45 St Stephen’s Green,
Dublin 2,
Ireland
22nd August 2013
John M Monaghan MB, FRCS(Ed), FRCOG
SUMMARY CV
My name is Mr. John M Monaghan, Consultant Gynaecological Oncologist; I was Director of Gynaecological Oncology Services at the Regional Department of Gynaecological Oncology at the Queen Elizabeth Hospital at Gateshead, 1978 – 1999. I was a Senior Lecturer in Gynaecological Oncology at the University of Newcastle upon Tyne and had been in this post for 28 years until I retired in June 2002.
I have published extensively on all aspects of Gynaecological Oncology, and have written over 42 chapters and text books on Gynaecological Oncology subjects and recently have published with Professor Albert Singer a text book on Colposcopy, Lower Genital Tract Precancer, an Atlas of Colposcopy (First and Second Editions), and also Co-Editor with John Shepherd of Clinical Gynaecological Oncology, First and Second Edition. I have edited Bonney's Gynaecological Surgery, Ninth and Tenth editions. Eleventh edition published February 2011. I am co-editor of 'An Atlas of Gynaecological Oncology', first and second editions, third edition published May 2011. It has now been commended in the BMA Book Awards 2012.
I have carried out a wide range of surgical and gynaecological oncology procedures over 28 years. During the 1990's I extended my laparoscopic experience, which began in 1968, into the area of advanced minimal access surgery, now having an extremely large experience of laparoscopic assisted vaginal hysterectomy and the wide range of radical laparoscopic procedures in gynaecological oncology. I have written extensively and lectured on gynaecological surgery in all its forms around the world.
I was a founding member of the British Gynaecological Cancer Society and held a number of offices as well as being a Council member for some years. I was a founding member of the International Gynaecological Cancer Society and have been Membership Secretary, a member of Council, and Vice-President. I am an honorary member of the Felix Rutledge Society, Member of Society of Pelvic Surgeons and Member of Society of Gynaecological Oncologists, all U.S. Societies.
I was appointed the RCOG Sims Black Visiting Professor for the year 2001 to visit the Far East. I was appointed Lead Clinician for the National Cancer Services Collaborative, Modernisation Agency, 2001.
In June 2002 I retired from Clinical work in the NHS but continued as National Clinical Lead for the Cancer Services Collaborative until June 2003. In 2003 I was registered with the Italian Medical Council and have been teaching surgery and setting up Multidisciplinary Treatment programmes in Emilia Romagna until September 2004.
GMC Registered Number: 0551609
MDU Number: 075565E
I am asked by David Harris Solicitor to prepare a report in the matter of Mrs Maureen Desmond - Date of Birth: 26.06.1937 concerning her care at Mater Hospital Dublin. I understand my overriding duty in writing this report is to assist the Court on matters which are within my expertise and I also understand that this duty overrides any obligation to David Harris (Solicitors) or their client.
I understand that my overriding duty in writing this report is to assist the court on matters within my expertise and that this duty overrides any obligation to David Harris, Solicitor or their clients. I confirm that I have complied with that duty and will continue to do so and that I am aware of the requirements set out in Part 35 of the Civil Procedure Rules and the accompanying Practice Direction, the Protocol for Instruction of Experts to give evidence in Civil Claims and the relevant Pre-action Practice Direction/Protocol.
I confirm that I have made clear which facts and matters referred to in this report are within my own knowledge and which are not. Those that are within my own knowledge I confirm to be true. The opinions I have expressed represent my true and complete professional opinions on the matters to which they refer.
22nd August 2013
MEDICAL REPORT
Documentation
I have available to me:
1 A detailed chronology prepared by Mr Stephen Desmond to include Mater Gynaecology notes, Letters of Complaint to the Mater Hospital, The General Medical Council Ireland, Letters from Mr W Boyd, A summary report from [The] London Clinic.
2 Records of the final hospital admission under Dr Lambert and Medical Oncology records.
History and Chronology.
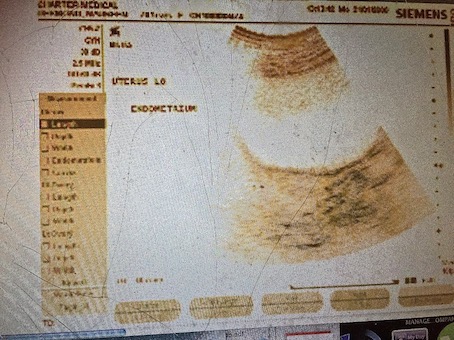
1.Mrs Maureen Desmond was a healthy lady of seventy when in November 2007 she was referred by her GP to the Mater Hospital rapid access clinic because she was complaining of abdominal discomfort and a clear profuse vaginal discharge. At the clinic visit on the 8th of November 2007 a CT scan was organised after examination had not revealed any significant findings apart from a large incisional hernia in the abdominal wall. The CT scan result showed an enlarged uterus and an endometrial thickness of 14 mm, described as heterogenous in the report; (an acceptable upper limit for the endometrium in a seventy year old is approximately 4 mm). An Ultra sound scan was then organised which confirmed the enlargement of the uterus and the endometrial thickness was identified as 13.7 mm. Again described as heterogenous. The ovaries were described as normal.
Comment; Such a finding in a post menopausal patient should generate an appointment within two weeks of the GP letter
3 Mrs Desmond and her son were alerted by the ultrasonographer to the importance of dealing with this situation and she was immediately referred to a gynaecologist, Mr William Boyd at the Mater hospital. In spite of the importance of the findings there was a large delay in achieving this first consultation which took place in 9th of April 2008. The letter written by Mr Boyd dated the 9th of April 2008 to the GP Dr Mary Chambers states the findings of the scans and notes the thickened endometrium and recommends a hysteroscopy and D&C. He Notes that she is 70 and diabetic and will need a pre-operative assessment.
4 Comment; the approach recommended is standard and should be instituted within two to four weeks of this consultation. In fact after prompting by the family an arrangement for an out patient hysteroscopy and Pipelle sample was made for 13th of August 2008. This is some nine months after the original referral and the worrying changes identified on the CT Scan and the ultra sound scan.
5 The procedure of Outpatient Hysteroscopy and Pipelle sample was carried out by Dr Moses on the 13th of August. The operation note is available and reads as ‘Hysteroscopy’
Under description of operation Dr Moses writes C/O Thickened endometrium on USS, No Symptoms.
O/E Abd Soft, NE N(ringed), size of A/V uterus. ( this means a normal sized uterus leaning forwards) Adnexae NAD, (this means ovaries and tubes were normal). Cx ….. ( not decipherable).
Hysteroscopy- moderate view.
N (ringed) Cavity. (means normal cavity)
L ostia seen, (the hole at the cornua of the uterus seen)
R ostia NAD ( I am not sure why a different comment is made here)
No Lesion.
Pipelle attempted, no sample as atrophic cavity.
Please discharge TCI, ( to come in ), if pv (per vagina) bleeding
Signed Moses
6 It is quite alarming that Dr Moses appears to be willing to ignore the findings of a CT Scan and an Ultra sound Scan and rely on what is clearly an unsatisfactory procedure where he has failed to identify an enlarged uterus, has mistaken a markedly thickened endometrium for an atrophic one and having in his own words ‘attempted’ a pipelle sample and failed. His decision to discharge the patient in the face of significant worrying findings is in my view so substandard as to be negligent.
7 At the very least a review of the patient should be arranged and a formal Hysteroscopy and D&C as advised by Mr Boyd should be carried out. The Pipelle sampler relies on suction to draw in a sample of endometrium into its cavity which is removed as the sampler is withdrawn. If the clinician does not perform the procedure correctly no sample will be produced. It is unacceptable to presume that because no sample has been obtained that the endometrium must be atrophic. This is particularly so when there is evidence on two different scans that there is marked thickening of the endometrium. It is clear in the light of subsequent developments that Dr Moses performed duties in an incompetent manner, including mis-assessing the size of the uterus at initial examination.
8. Sadly the news that there was no problem was received by Mrs Desmond and her son and no further action took place until Mrs Desmond began to bleed vaginally and was referred back to the hospital where seen by Mr Boyd in July 2010 when Hysteroscopy and D&C performed under general anaesthetic revealed an obvious cancer of the uterine cavity. The procedure which should have been done some two years previously was performed under general anaesthetic without any problem. A high grade papillary serous endometrial cancer was identified. Later on the 22nd of July 2010 a fine needle aspiration of an ‘omental node’, was taken which showed infiltration with the same cancer, that is the cancer had spread to the peritoneal cavity and was inoperable. A CT Scan confirmed abdominal disease at this time.
9.On the 22nd of December a PET Scan confirmed residual disease in the uterus and in the abdominal cavity. Curiously in a letter dated 15th of December 2010 Mr Boyd wrote to Dr Noeleen Gleeson a consultant gynaecologist at the St James’ Hospital Dublin asking for a second opinion. He notes that Mrs Desmond had had symptoms of discharge and had a hysteroscopy ‘but unfortunately did not have a D&C at the time’. Mr Boyd somewhat disingenuously does not mention that this missed opportunity was some two years before the eventual diagnosis. He then goes on to describe an ‘ovarian cancer’ which had been treated with three cycles of chemotherapy but with little response. This is not borne out by the scans which show a 25% reduction. He asks Dr Gleeson to consider surgery as an interval procedure.
10. Comment; There seems to have been some curious changes in opinions about the fitness or other wise of Mrs Desmond to survive surgery. One minute she is too unfit for a Hysteroscopy and D&C and next has a Hysteroscopy and D&C and now is being considered for extensive debulking surgery.
11. On the 3rd of December 2010 Mrs Desmond GP Dr Chambers writes to Medical records at the Mater Hospital asking if she could have a copy of the letter and notes relating to the admission of 13.08.08
12.Attempts were made to treat Mrs Desmond with chemotherapy but she had adverse reactions including Staphylococcal infection in her port and possible excessive dosage of chemotherapeutic agents. These problems are the subject of a separate complaint from Mr Stephen Desmond. These complications resulted in prolonged hospitalisation. No further action took place in terms of active treatment and Mrs Desmond was looked after by the palliative care team who seemed to labour under the misapprehension that the patient had an ovarian cancer.
13. Eventually Mrs Desmond was admitted to hospital through A&E To the Mater hospital with shortage of breath. She died of a pulmonary embolus on the 4th of September 2011. Her care in this last episode is the subject of a separate complaint from Mr Stephen Desmond.
14. A Coroner’s post mortem was carried out which confirmed the cause of death to be a Pulmonary embolus secondary to metastatic endometrial adenocarcinoma. Both ovaries were described as normal by the pathologist.
15.Mr Stephen Desmond has made representations to the General Medical council concerning the standard of care given to his mother by Mr Boyd, Dr Lambert and Professor McCaffrey.
Summary. Any woman aged 70 presenting to her doctor with a significant new discharge from the vagina whether accompanied by bleeding or not should be treated as an urgent and concerning case. The initial care of Mrs Desmond was correct as an Ultrasound of the pelvis and CT scan was organised. The ultrasound is the diagnostic tool of choice in these circumstances and it showed an endometrium 13.7 mm thick demonstrating heterogenous patterns. This report quite rightly rang alarm bells and an appointment was made to see a gynaecologist, ( Mr W Boyd)
The gynaecologist was also stimulated by the unusual and concerning findings on the ultrasound and CT Scan to organise a Hysteroscopy and a D&C.. This procedure should have been performed as a matter of urgency within the next four weeks. For whatever reason Mrs Desmond was not brought in for the procedure until nine months later. This is not acceptable practice and is negligent
The procedure was also translated into an Outpatient Hysteroscopy and Pipelle sample. Such a procedure is often very difficult for the doctor and uncomfortable for the patient. The procedure was also done by a junior doctor. This would have been acceptable if that person had been supervised and his/her findings checked. From Mr Desmond’s communication to me it would appear that there was difficulty in visualising the screen due to incident light and the junior doctor made the diagnosis of an atrophic endometrium and no Pipelle sample was obtained. In the operation record Dr Moses records that a ‘Pipelle sample was attempted’.
Mr Desmond was then discharged from the clinic without a diagnosis, without any explanation for the conflicting findings on Ultrasound/CT Scan and hysteroscopy, and without any arrangement for review to either resolve this conflict or to identify other investigation or to proceed to the original proposed Hysteroscopy and D&C.
In the event two years later the patient was identified with inoperable uterine cancer and died one year thereafter..
Comment.
The initial phases of this case were well managed.
1/. The Ultrasound and CT scans were appropriate investigations.
2/. Once an abnormality had been identified in the endometrium referral to a gynaecologist was correct and the organisation of a Hysteroscopy and D&C was correct.
To perform the procedure some nine months later was unacceptable and negligent.
3/.Changing the procedure to an outpatient Hysteroscopy and Pipelle sample was acceptable so long as a good view of the interior of the uterus could be seen and a confident Pipelle sample produced. In these circumstances of an ‘unsatisfactory test’. A move to a formal Hysteroscopy and D&C under anaesthetic was mandatory. Not to do so is substandard and negligent
4/. If a further procedure had not been organised a review of the case should have been performed to determine why there was a discrepancy between the ultrasound/CT Scan result and the findings at Hysteroscopy. Not to do so is substandard and negligent. A repetition of the ultrasound would have been a minimal requirement.
5/. To discharge the patient without any review of either the case or the patient is substandard and negligent.
6/. In my view there was clear evidence of a breach of duty of care in this case. In causation terms, if Mrs Desmond had had a diagnosis of her uterine cancer made some one year and eight months prior to its eventual diagnosis she would have had a simple procedure such as a total hysterectomy with removal of ovaries and on the balance of probabilities would have been cured of her cancer. Uterine cancer has a very high cure rate when the cancer is diagnosed within the confines of the uterus but the cure rates drop rapidly when spread has occurred outside the uterus. It is a pity that the opportunity to diagnose this cancer at an eminently curable phase was lost due to the failings of the Mater Hospital and its staff .
Statement of Truth
I confirm that I have made clear which facts and matters referred to in this report are within my own knowledge and which are not. Those that are within my own knowledge I confirm to be true. The opinions I have expressed represent my true and complete professional opinions on the matters to which they refer.
Signed ………………………….
J M Monaghan
Date: 22nd August 2013
*****************************************************************************
FURTHER MEDICAL REPORTS
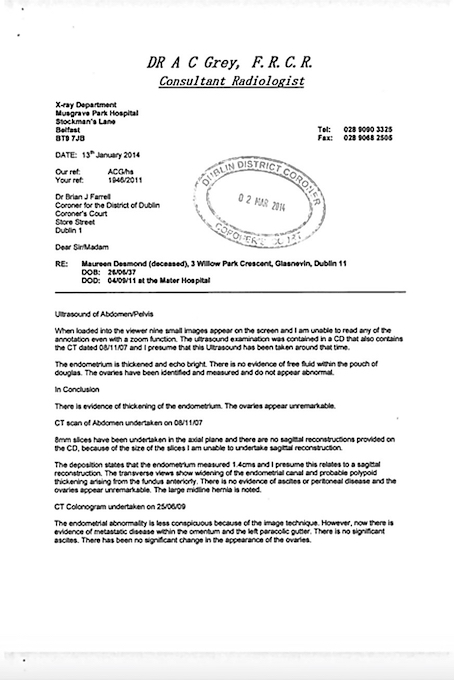
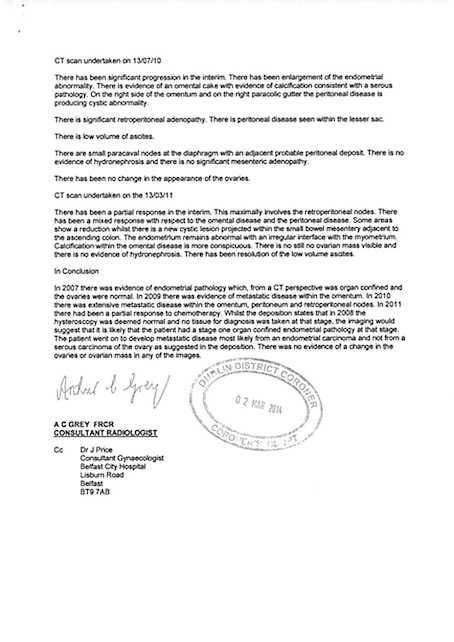
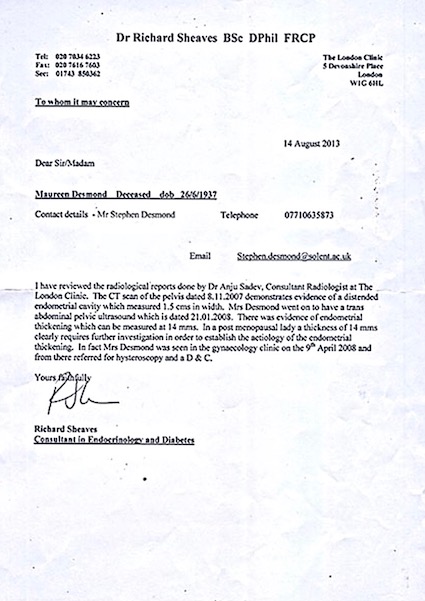
1) 13th January 2014: The Coroner's review of Maureen Desmond's Radiology which confirms a Stage I pathology when Maureen was discharged from The Mater without a biopsy in August 2008, and cancer on the CT scan of June 2009 which was read at The Mater as "normal"
The reports below were written by Charter Medical Dublin and The London Clinic on Harley Street. Charter Medical reviewed their original scans on Maureen of January 2008---Charter Medical confirmed and have stood over their original findings, i.e. a 14mm thickened endometrium, abnormal distended uterine cavity, and enlarged uterus. The London Clinic also reviewed the original scans and reports, fully agreed with Charter Medical, and confirmed an endometrial thickening of 14mm, distended uterine cavity, etc. According to Dr. Monaghan's expert report, these findings on the original scans contradict the finding made by The Mater's Gynaecology Registrar when he discharged Maureen from The Mater Gynaecology Clinic after hysteroscopy and without a biopsy in August 2008. The Gynaecology Registrar at The Mater wrote that he could not obtain a biopsy sample because of endometrial atrophy (an ultra thin lining of the endometrium)--However, a frame (immediately below) from the original ultrasound in question does NOT show atrophy--it shows a gross thickening of the endometrium, according to Charter Medical and The London Clinic. The coroner, having considered all of the depositions, and witness statements and evidence provided, ruled that this treatment episode was a missed opportunity to diagnose Maureen with cancer.
There is no explanation as to how The Mater's Gynaecology Registrar mistook (according to Dr. Monaghan), on hysteroscopic view, a grossly thickened 14mm endometrium for an ultra-thin atrophic endometrium, other than the evidence given by Maureen's son to the inquest into her death. At the inquest Maureen Desmond's son stated that he was present outside the examination room when The Mater's Gynaecology Registrar performed the hysteroscopy and Stephen heard the nurse saying to him "Doctor, we can't see the screen...will I pull the blind". Stephen Desmond then testified that The Mater's Gynaecology Registrar replied "No".
DISCLAIMER: September 2014.
All third-party documents included on the website, including third-party medical reports, newspaper articles, television segments, etc. are provided for research purposes only, and while every attempt is made to ensure they are fully accurate, anyone reading this website should not infer any guarantee by the author of this website with regard to the accuracy of third party materials contained here, and understand that these materials are provided purely for research (including academic research) archive and reference purposes for those who have an interest in compelling gynaecological cases in Ireland and how they have been documented, written about, and studied by others. This website should not be considered 'investigative' or 'expose'. Equally, any reader of this website should not infer that quotations of this website's author (including The Centre for Conflict Resolution Journalism and any of its Directors or agents) in relation to this story in any third party materials included on this website, or in any other materials in the public domain (including newspaper articles, etc), are accurate without first confirming such directly in writing with the author of this website. The inclusion of third party materials on this website which contain quotations from the author of this website (or its directors) , does not infer in any way that the author of this website, or CCRJ directors agree that these quotations are accurate. All materials are provided on this website for research, archive and reference purposes only, to give a sample of the materials that have been produced by third parties in relation to this story, and their inclusion does not infer the agreement of author of this website as to the ultimate accuracy of these materials, now or in the future, or as may be determined by any process including medical-clinical negligence proceedings in front of The High Court, etc. Having said all of that, every effort is made to ensure the accuracy of all materials contained here, but be advised this disclaimer operates into perpetuity.
This website, from the date of creation in 2014, is owned, authored, managed and operated by The Centre for Conflict Resolution Journalism, Limited, a company registered in Northern Ireland with Limited Liability. All statements made on this website, including statements attributed to CCRJ Directors in third party materials, are attributable to the CCRJ with the provisos and conditions contained herein and above. This website www.maureendesmond.com is a continuation of the company website www.ccrj.org
These websites support the professional services of the CCRJ. The CCRJ is an academic research centre and from time to time produces sister websites to www.ccrj.org which highlight research projects, including practice-based research projects on relevant topics, case studies, individual stories and social issues which form the basis of CCRJ academic research projects.
This website is authored on behalf of the CCRJ, and the CCRJ bears all and sole liability for content of the website contained herein.
The Maureen Desmond Foundation is a programme of The Centre for Conflict Resolution Journalism--a limited liability company registered in Northern Ireland dedicated to education and research.